
Pale Blue Dot
Live a healthier life, avoid cancer, heart issues, diabetes and arthritis and other autoimmune diseases.

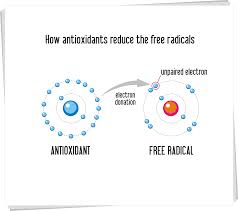
Antioxidants are phytochemicals, vitamins and other nutrients that protect our cells from damage caused by free radicals. In vitro en in vivo studies have shown that antioxidants help prevent the free radical damage that is associated with cancer and heart disease. Antioxidants can be found in most fruits and vegetables but also culinary herbs and medicinal herbs can contain high levels of antioxidants. Dragland S and colleagues showed in their study entitled “Several Culinary and Medicinal Herbs are Important Sources of Dietary Antioxidants”, and published in the Journal of Nutrition (2003 May) that the antioxidant level of herbs can be as high as 465 mmol per 100 g. A study in 2006 by Thompson HJ showed that a botanical diversity of fruits and vegetables plays a role in the biological effect of antioxidant phytochemicals. The consumption of smaller quantities of many phytochemicals may result in more health benefits than the consumption of larger quantities of fewer phytochemicals. What are free radicals?Free radicals are formed as part of our natural metabolism but also by environmental factors, including smoking, pesticides, pollution and radiation. Free radicals are unstable molecules which react easily with essential molecules of our body, including DNA, fat and proteins. All organic and inorganic materials consist of atoms, which can be bound together to form molecules. Each atom has a specific number of protons (positively charged) and electrons (negatively charged). Most single atoms are not stable because they have to few or to may electrons. Atoms try to reach a state of maximum stability by giving away or receiving electrons from other atoms, thereby forming molecules. Free radicals are molecules which have one electron too much or too less in order to be stable. Free radicals try to steal or give electrons to other molecules, thereby changing their chemical structure. When a free radical attacks a molecule, it will then become a free radical itself, causing a chain reaction which can result in the destruction of a cell. Antioxidants have the property to neutralize free radicals without becoming a free radicals themselves. When antioxidants neutralize free radicals by receiving or donating an electron they do not become antioxidants themselves because they are stable in both forms. In other words, antioxidants are chemicals that offer up their own electrons to the free radicals, thus preventing cellular damage. However, when the antioxidant neutralizes a free radical it becomes inactive. Therefore we need to continuously supply our body with antioxidants. The action of free radicals could increase the risk of diseases such as cancer and hearth problems and could accelerate ageing. Antioxidants have the property to neutralize the free radicals and prevent damage. Well known examples of antioxidants are the vitamin C, E and beta-carotene. These three vitamins are often added to the so called ACE drinks. But there are numerous other rather unknown antioxidants such as lycopene, lutein, Benefits of antioxidantsNumerous studies with plant phytochemicals show that phytochemicals with antioxidant activity may reduce risk of cancer and improve heart health. Antioxidants reduce the risk of cancerNot all results are conclusive but many studies show that antioxidants may reduce the risk of cancer. A large randomized trial on antioxidants and cancer risk was the Chinese Cancer Prevention Study (1993). This study showed that a combination of the antioxidants beta-carotene, vitamin E and selenium significantly reduced incidence of cancer. However, the Alpha-Tocopherol / Beta-Carotene Cancer Prevention Study (1994) showed that intake of beta-carotene increased lung cancer rates of male smokers. Antioxidants protect the heartEveryone knows that cholesterol causes heart diseases and tries to limit cholesterol intake. But a more important cause of fatty buildups in the arteries is the oxidation of low-density lipoprotein cholesterol. The use of dietary supplements of antioxidants could reduce the risk of cardiovascular disease, but there is no hard evidence. At this stage, studies only show that the intake of foods, naturally rich in antioxidants reduces this risk |
AlkaloidsAnthocyaninsCarotenoidsCoumestansFlavan-3-OlsFlavonoids
Hydroxycinnamic AcidsIsoflavonesLignansMonophenols |
MonoterpenesOrganosulfidesOther PhytochemicalsPhenolic AcidsPhytosterolsSaponinsStylbenesTriterpenoidsXanthophylls |
VegetablesFruits and Nuts
Medicinal Plants |
Common Herbs
Beans and seeds |
| Phytochemicals |
|
|||||||||||||
English | Español
Vitamin B12 has the largest and most complex chemical structure of all thevitamins. It is unique among vitamins in that it contains a metal ion, cobalt. For this reason cobalamin is the term used to refer to compounds having vitamin B12activity. Methylcobalamin and 5-deoxyadenosylcobalamin are the forms of vitamin B12 used in the human body (1). The form of cobalamin used in most nutritional supplements and fortified foods, cyanocobalamin, is readily converted to 5-deoxyadenosylcobalamin and methylcobalamin in the body. In mammals, cobalamin is a cofactor for only two enzymes, methionine synthase and L-methylmalonyl-coenzyme A mutase (2).
Cofactor for methionine synthase
Methylcobalamin is required for the function of the folate-dependent enzyme, methionine synthase. This enzyme is required for the synthesis of the amino acid,methionine, from homocysteine. Methionine in turn is required for the synthesis of S-adenosylmethionine, a methyl group donor used in many biological methylationreactions, including the methylation of a number of sites within DNA, RNA, andproteins (3). Aberrant methylation of DNA and proteins, which causes alterations inchromatin structure and gene expression, are a common feature of cancer cells. Inadequate function of methionine synthase can lead to an accumulation of homocysteine, which has been associated with increased risk of cardiovascular diseases (diagram).
Cofactor for L-methylmalonyl-coenzyme A mutase
5-Deoxyadenosylcobalamin is required by the enzyme that catalyzes the conversion of L-methylmalonyl-coenzyme A to succinyl-coenzyme A (succinyl-CoA), which then enters the citric acid cycle (see diagram). Succinyl-CoA plays an important role in the production of energy from lipids and proteins and is also required for thesynthesis of hemoglobin, the oxygen-carrying pigment in red blood cells (3).
In healthy adults, vitamin B12 deficiency is uncommon, mainly because total body stores can exceed 2,500 mcg, daily turnover is slow, and dietary intake of only 2.4 mcg/day is sufficient to maintain adequate vitamin B12 status (see RDA below) (4). In elderly individuals, vitamin B12 deficiency is more common mainly because of impaired intestinal absorption that can result in marginal to severe vitamin B12deficiency in this population.
Causes of vitamin B12 deficiency
Intestinal malabsorption, rather than inadequate dietary intake, can explain most cases of vitamin B12 deficiency (5). Absorption of vitamin B12 from food requires normal function of the stomach, pancreas, and small intestine. Stomach acid andenzymes free vitamin B12 from food, allowing it to bind to R-protein (also known as transcobalamin-1 or haptocorrin), found in saliva and gastric fluids. In the alkalineenvironment of the small intestine, R-proteins are degraded by pancreatic enzymes, freeing vitamin B12 to bind to intrinsic factor (IF), a protein secreted by specialized cells in the stomach. Receptors on the surface of the ileum (final part of the small intestine) take up the IF-B12 complex only in the presence of calcium, which is supplied by the pancreas (5). Vitamin B12 can also be absorbed by passive diffusion, but this process is very inefficient—only about 1% absorption of the vitamin B12dose is absorbed passively (2). The prevalent causes of vitamin B12 deficiency are (1) an autoimmune condition known as pernicious anemia, and (2) a disorder called food-bound vitamin B12 malabsorption. Both conditions have been associated with a chronic inflammatory disease of the stomach known as atrophic gastritis.
Atrophic gastritis is thought to affect 10%-30% of people over 60 years of age (6). The condition is frequently associated with the presence of autoantibodies directed towards stomach cells (see Pernicious anemia) and/or infection by the bacteria,Helicobacter pylori (H. pylori) (7). H. pylori infection induces chronic inflammation of the stomach, which may progress to peptic ulcer disease, atrophic gastritis, and/orgastric cancer in some individuals. Diminished gastric function in individuals with atrophic gastritis can result in bacterial overgrowth in the small intestine and cause food-bound vitamin B12 malabsorption. Vitamin B12 levels in serum, plasma, and gastric fluids are significantly decreased in individuals with H. pylori infection, and eradication of the bacteria has been shown to significantly improve vitamin B12serum concentrations (8).
Pernicious anemia has been estimated to be present in approximately 2% of individuals over 60 years of age (9). Although anemia is often a symptom, the condition is actually the end stage of an autoimmune inflammation of the stomach known as autoimmune atrophic gastritis, resulting in destruction of stomach cells by one’s own antibodies (autoantibodies). Progressive destruction of the cells that line the stomach causes decreased secretion of acid and enzymes required to release food-bound vitamin B12. Antibodies to intrinsic factor (IF) bind to IF preventing formation of the IF-B12 complex, further inhibiting vitamin B12 absorption. About 20% of the relatives of pernicious anemia patients also have the condition, suggesting a genetic predisposition. It is also thought that H. pylori infection could be involved in initiating the autoimmune response in a subset of individuals (10). Further, co-occurrence of autoimmune atrophic gastritis with other autoimmune conditions, especially autoimmune thyroiditis and type 1 diabetes mellitus, has been reported (11, 12).
Treatment of pernicious anemia generally requires injections of vitamin B12 to bypass intestinal absorption. High-dose oral supplementation is another treatment option, because consuming 1,000 mcg (1 mg)/day of vitamin B12 orally should result in the absorption of about 10 mcg/day (1% of dose) by passive diffusion. In fact, high-dose oral therapy is considered to be as effective as intramuscular injection(4).
Food-bound vitamin B12 malabsorption
Food-bound vitamin B12 malabsorption is defined as an impaired ability to absorb food- or protein-bound vitamin B12; individuals with this condition can fully absorb the free form (13). While the condition is the major cause of poor vitamin B12 status in the elderly population, it is usually associated with atrophic gastritis, a chronicinflammation of the lining of the stomach that ultimately results in the loss of glands in the stomach (atrophy) and decreased stomach acid production (see Atrophic gastritis above). Because stomach acid is required for the release of vitamin B12from the proteins in food, vitamin B12 absorption is diminished. Decreased stomach acid production also provides an environment conducive to the overgrowth ofanaerobic bacteria in the stomach, which further interferes with vitamin B12absorption (3). Because vitamin B12 in supplements is not bound to protein, and because intrinsic factor (IF) is still available, the absorption of supplemental vitamin B12 is not reduced as it is in pernicious anemia. Thus, individuals with food-bound vitamin B12 malabsorption do not have an increased requirement for vitamin B12; they simply need it in the crystalline form found in fortified foods and dietary supplements.
Other causes of vitamin B12 deficiency
Other causes of vitamin B12 deficiency include surgical resection of the stomach or portions of the small intestine where receptors for the IF-B12 complex are located. Conditions affecting the small intestine, such as malabsorption syndromes (celiac disease and tropical sprue), may also result in vitamin B12 deficiency. Because thepancreas provides critical enzymes, as well as calcium required for vitamin B12absorption, pancreatic insufficiency may contribute to vitamin B12 deficiency. Since vitamin B12 is found only in foods of animal origin, a strict vegetarian (vegan) diet has resulted in cases of vitamin B12 deficiency. Moreover, alcoholics may experience reduced intestinal absorption of vitamin B12 (2), and individuals with acquired immunodeficiency syndrome (AIDS) appear to be at increased risk of deficiency, possibly related to a failure of the IF-B12 receptor to take up the IF-B12 complex(3). Further, long-term use of acid-reducing drugs has also been implicated in vitamin B12 deficiency (see Drug interactions).
Inherited disorders of vitamin B12 absorption
Rare cases of inborn errors of vitamin B12 metabolism have been reported in the literature (reviewed in 5). Imerslund-Gräsbeck syndrome is an inherited vitamin B12malabsorption syndrome that causes megaloblastic anemia and neurologic disorders of variable severity in affected subjects. Similar clinical symptoms are found in individuals with hereditary IF deficiency (also called congenital pernicious anemia) in whom the lack of IF results in the defective absorption of vitamin B12. Additionally,mutations affecting vitamin B12 transport in the body have been identified (14).
Symptoms of vitamin B12 deficiency
Vitamin B12 deficiency results in impairment of the activities of vitamin B12-requiring enzymes. Impaired activity of methionine synthase results in elevatedhomocysteine levels, while impaired activity of L-methylmalonyl-CoA mutase results in increased levels of a metabolite of methylmalonyl-CoA called methylmalonic acid (MMA). While individuals with mild vitamin B12 deficiency may not experience symptoms, blood levels of homocysteine and/or MMA may be elevated (15).
Megaloblastic anemia
Diminished activity of methionine synthase in vitamin B12 deficiency inhibits the regeneration of tetrahydrofolate (THF) and traps folate in a form that is not usable by the body (see diagram), resulting in symptoms of folate deficiency even in the presence of adequate folate levels. Thus, in both folate and vitamin B12 deficiencies, folate is unavailable to participate in DNA synthesis. This impairment of DNA synthesis affects the rapidly dividing cells of the bone marrow earlier than other cells, resulting in the production of large, immature, hemoglobin-poor red blood cells. The resulting anemia is known as megaloblastic anemia and is the symptom for which the disease, pernicious anemia, was named (3). Supplementation with folic acid will provide enough usable folate to restore normal red blood cell formation. However, if vitamin B12 deficiency is the cause, it will persist despite the resolution of the anemia. Thus, megaloblastic anemia should not be treated with folic acid until the underlying cause has been determined (16).
Neurologic symptoms
The neurologic symptoms of vitamin B12 deficiency include numbness and tingling of the hands and, more commonly, the feet; difficulty walking; memory loss; disorientation; and dementia with or without mood changes. Although the progression of neurologic complications is generally gradual, such symptoms may not be reversed with treatment of vitamin B12 deficiency, especially if they have been present for a long time. Neurologic complications are not always associated with megaloblastic anemia and are the only clinical symptom of vitamin B12deficiency in about 25% of cases (17). Although vitamin B12 deficiency is known to damage the myelin sheath covering cranial, spinal, and peripheral nerves, the biochemical processes leading to neurological damage in vitamin B12 deficiency are not yet fully understood (18).
Gastrointestinal symptoms
Tongue soreness, appetite loss, and constipation have also been associated with vitamin B12 deficiency. The origins of these symptoms are unclear, but they may be related to the stomach inflammation underlying some cases of vitamin B12deficiency and to the progressive destruction of the lining of the stomach (17).
The Recommended Dietary Allowance (RDA)
The RDA for vitamin B12 was revised by the Food and Nutrition Board (FNB) of the US Institute of Medicine in 1998. Because of the increased risk of food-bound vitamin B12 malabsorption in older adults, the FNB recommended that adults over 50 years of age get most of the RDA from fortified food or vitamin B12-containing supplements (17).
| Recommended Dietary Allowance (RDA) for Vitamin B12 | |||
| Life Stage | Age | Males (mcg/day) | Females (mcg/day) |
| Infants | 0-6 months | 0.4 (AI) | 0.4 (AI) |
| Infants | 7-12 months | 0.5 (AI) | 0.5 (AI) |
| Children | 1-3 years | 0.9 | 0.9 |
| Children | 4-8 years | 1.2 | 1.2 |
| Children | 9-13 years | 1.8 | 1.8 |
| Adolescents | 14-18 years | 2.4 | 2.4 |
| Adults | 19-50 years | 2.4 | 2.4 |
| Adults | 51 years and older | 2.4* | 2.4* |
| Pregnancy | all ages | – | 2.6 |
| Breast-feeding | all ages | – | 2.8 |
*Vitamin B12 intake should be from supplements or fortified foods due to the age-related increase in food-bound malabsorption.
As mentioned above, chronic atrophic gastritis and infection by H. pylori can cause deficiency in vitamin B12 secondary to malabsorption disorders (see Causes of vitamin B12 deficiency). However, the occurrence of H. pylori infection and chronic atrophic gastritis did not modify the five-year incidence of cardiovascular accidents (stroke and heart attack) or mortality in a large cohort study of nearly 10,000 men and women over 50 years old (19). Yet, vitamin B12 status was not assessed in this study, despite the high prevalence of vitamin B12 deficiency in older individuals.
Homocysteine and cardiovascular diseases
Epidemiological studies indicate that even moderately elevated levels ofhomocysteine in the blood raise the risk of cardiovascular diseases (CVD) (20), though the mechanism by which homocysteine may increase the CVD risk remains the subject of a great deal of research (21). The amount of homocysteine in the blood is regulated by at least three vitamins: folate, vitamin B6, and vitamin B12(see diagram). An early analysis of the results of 12 randomized controlled trialsshowed that folic acid supplementation (0.5-5 mg/day) had the greatest lowering effect on blood homocysteine levels (25% decrease); co-supplementation with folic acid and vitamin B12 (500 mcg/day) provided an additional 7% reduction (32% decrease) in blood homocysteine concentrations (22). The results of a sequential supplementation trial in 53 men and women indicated that after folic acid supplementation, vitamin B12 became the major determinant of plasmahomocysteine levels (23). It is thought that the elevation of homocysteine levels might be partly due to vitamin B12 deficiency in individuals over 60 years of age. Two studies found blood methylmalonic acid (MMA) levels to be elevated in more than 60% of elderly individuals with elevated homocysteine levels. In the absence of impaired kidney function, an elevated MMA level in conjunction with elevated homocysteine suggests either a vitamin B12 deficiency or a combined vitamin B12and folate deficiency (24). Thus, it appears important to evaluate vitamin B12status, as well as kidney function, in older individuals with elevated homocysteine levels prior to initiating homocysteine-lowering therapy. For more information regarding homocysteine and CVD, see the article on folate.
Intervention studies
Although increased intake of folic acid and vitamin B12 is effective in decreasinghomocysteine levels, the combined intervention of these B vitamins did not lower risk for CVD. Indeed, several randomized, placebo-controlled trials have been conducted to determine whether homocysteine-lowering through folic acid, vitamin B12, and vitamin B6 supplementation reduces the incidence of CVD. A recent meta-analysis of data from 11 trials, including nearly 45,000 participants at risk of CVD, showed that B-vitamin supplementation had no significant effect on risk ofmyocardial infarction (heart attack) or stroke, nor did it modify the risk of all-cause mortality (25). Other meta-analyses that included patients with chronic kidney disease have confirmed the lack of effect of homocysteine-lowering on risk of myocardial infarction and death. However, stroke risk was significantly reduced by 7%-12% with the B-vitamin supplementation (26, 27). Another meta-analysis of 12clinical trials measuring flow-mediated vasodilation (FMD; a surrogate marker of vascular health) in response to homocysteine reduction revealed that B-vitamin supplementation was accompanied by an improved FMD in short-term <8 weeks) but not in long-term studies conducted in subjects with preexisting vascular diseases (28). Yet, some of the studies included in these meta-analyses did not use vitamin B12, and folate administration on its own has shown a protective role on vascular function and stroke risk (29). Besides, the high prevalence ofmalabsorption disorders and vitamin B12 deficiency in elderly individuals might warrant the use of higher doses of vitamin B12 than those used in these trials (30); in cases of malabsorption, only high-dose oral therapy or intramuscular injections can overcome vitamin B12 deficiency (4).
Folate is required for synthesis of DNA, and there is evidence that decreased availability of folate results in strands of DNA that are more susceptible to damage. Deficiency of vitamin B12 traps folate in a form that is unusable by the body for DNA synthesis. Both vitamin B12 and folate deficiencies result in a diminished capacity formethylation reactions (see diagram). Thus, vitamin B12 deficiency may lead to an elevated rate of DNA damage and altered methylation of DNA, both of which are important risk factors for cancer. A series of studies in young adults and older men indicated that increased levels of homocysteine and decreased levels of vitamin B12in the blood were associated with a biomarker of chromosome breakage in white blood cells (reviewed in 31). In a double-blind, placebo-controlled study, the same biomarker of chromosome breakage was minimized in young adults who were supplemented with 700 mcg of folic acid and 7 mcg of vitamin B12 daily in cereal for two months (32).
A case-control study compared prediagnostic levels of serum folate, vitamin B6, and vitamin B12 in 195 women later diagnosed with breast cancer and 195 age-matched, cancer-free women. Among postmenopausal women, the association between blood levels of vitamin B12 and breast cancer suggested a threshold effect. The risk of breast cancer was more than doubled in women with serum vitamin B12 levels in the lowest quintile compared to women in the four highest quintiles (33). However, the meta-analysis of this study with three additional case-control studies found no protection associated with high compared to low vitamin B12 serum levels (34). A case-control study in Mexican women (475 cases and 1,391 controls) reported that breast cancer risk for women in the highest quartile of vitamin B12 intake (7.3-7.7 mcg/day) was 68% lower than those in the lowest quartile (2.6 mcg/day). Stratification of the data revealed that the inverse association between dietary vitamin B12 intake and breast cancer risk was stronger in postmenopausal women compared to premenopausal women, though both associations were statistically significant. Moreover, among postmenopausal women, the apparent protection conferred by folate was only observed in women with the highest vitamin B12quartiles of intake (35). However, more recent case-control and prospective cohort studies have reported weak to no risk reduction with vitamin B12 intakes in different populations, including Hispanic, African American and European American women (36, 37). A meta-analysis of seven case-control and seven prospective cohort studies concluded that the risk of breast cancer was not modified by high versus low vitamin B12 intakes (34). There was no joint association between folate and vitamin B12 intakes and breast cancer risk. Presently, there is little evidence to suggest a relationship between vitamin B12 status and breast cancer. In addition, results from observational studies are not consistently in support of an association between high dietary folate intakes and reduced risk for breast cancer (see the article on Folate). There is a need to evaluate the effect of folate and vitamin B12supplementation in well-controlled, randomized, clinical trials, while considering various factors that modify breast cancer risk, such as menopausal status, ethnicity, and alcohol intake.
Neural tube defects (NTD) may result in anencephaly or spina bifida, which are mostly fatal congenital malformations of the central nervous system. The defects arise from failure of embryonic neural tube to close, which occurs between the 21stand 28th days after conception, a time when many women are unaware of their pregnancy (38). Randomized controlled trials have demonstrated 60% to 100% reductions in NTD cases when women consumed folic acid supplements in addition to a varied diet during the month before and the month after conception. Increasing evidence indicates that the homocysteine-lowering effect of folic acid plays a critical role in reducing the risk of NTD (39). Homocysteine may accumulate in the blood when there is inadequate folate and/or vitamin B12 for effective functioning of the methionine synthase enzyme. Decreased vitamin B12 levels and elevated homocysteine concentrations have been found in the blood and amniotic fluid of pregnant women at high risk of NTD (40). The recent meta-analysis of 12 case-control studies, including 567 mothers with current or prior NTD-affected pregnancy and 1,566 unaffected mothers, showed that low maternal vitamin B12 status was associated with an increased risk of NTD (41). Yet, whether vitamin B12supplementation may be beneficial in the prevention of NTD has not been evaluated(42).
Cognitive decline, dementia, and Alzheimer’s disease
The occurrence of vitamin B12 deficiency prevails in the elderly population and has been frequently associated with Alzheimer’s disease (reviewed in 43). One study found lower vitamin B12 levels in the cerebrospinal fluid of patients with Alzheimer’s disease than in patients with other types of dementia, though blood levels of vitamin B12 did not differ (44). The reason for the association of low vitamin B12status with Alzheimer’s disease is not clear. Vitamin B12 deficiency, like folatedeficiency, may lead to decreased synthesis of methionine and S-adenosylmethionine (SAM), thereby adversely affecting methylation reactions. Methylation reactions are essential for the metabolism of components of the myelinsheath of nerve cells as well as for synthesis of neurotransmitters (18). Other metabolic implications of vitamin B12 deficiency include the accumulation of homocysteine and methylmalonic acid, which might contribute to the neuropathologic features of dementia (43).
Observational studies
A large majority of cross-sectional and prospective cohort studies have associated elevated homocysteine concentrations with measures of poor cognitive scores and increased risk of dementia, including Alzheimer’s disease (reviewed in 45). A case-control study of 164 patients with dementia of Alzheimer’s type included 76 cases in which the diagnosis of Alzheimer’s disease was confirmed by examination of brain cells after death. Compared to 108 control subjects without evidence of dementia, subjects with dementia of Alzheimer’s type and confirmed Alzheimer’s disease had higher blood homocysteine levels and lower blood levels of folate and vitamin B12. Measures of general nutritional status indicated that the association of increased homocysteine levels and diminished vitamin B12 status with Alzheimer’s disease was not due to dementia-related malnutrition (46). In a sample of 1,092 men and women without dementia followed for an average of 10 years, those with higherplasma homocysteine levels at baseline had a significantly higher risk of developing Alzheimer’s disease and other types of dementia. Specifically, those with plasma homocysteine levels greater than 14 micromol/L had nearly double the risk of developing Alzheimer’s disease (47). A study in 650 elderly men and women reported that the risk of elevated plasma homocysteine levels was significantly higher in those with lower cognitive function scores (48). A prospective study in 816 elderly men and women reported that those with hyperhomocysteinemia(homocysteine levels >15 micromol/L) had a significantly higher risk of developing Alzheimer’s disease or dementia. Although raised homocysteine levels might be partly due to a poor vitamin B12 status, the latter was not related to risk of Alzheimer’s disease or dementia in this study (49).
A recent systematic review of 35 prospective cohort studies assessing the association between vitamin B12 status and cognitive deterioration in older individuals with or without dementia at baseline did not support a relationship between vitamin B12 serum concentrations and cognitive decline, dementia, or Alzheimer’s disease (50). Nevertheless, studies utilizing more sensitive biomarkersof vitamin B12 status, including measures of holo-transcobalamin (holo-TC; a vitamin B12 carrier) and methylmalonic acid, showed more consistent results and a trend toward associations between poor vitamin B12 status and faster cognitive decline and risk of Alzheimer’s disease (51-55). Besides, it cannot be excluded that the co-occurrence of potential confounders like elevated homocysteine level and poor folate status might mitigate the true contribution of vitamin B12 status to cognitive functioning (45).
Intervention studies
High-dose B-vitamin supplementation has been proven effective for treatinghyperhomocysteinemia in elderly individuals with or without cognitive impairment. However, homocysteine-lowering trials have produced equivocal results regarding the prevention of cognitive deterioration in this population. A systematic review andmeta-analysis of 18 randomized, placebo-controlled trials examining the effect of B-vitamin supplementation did not find that the decrease in homocysteine level prevented or delayed cognitive decline among older subjects (56). A more recent randomized, double-blind, placebo-controlled clinical trial in 900 older individuals at high risk of cognitive impairment found that daily supplementation of 400 mcg of folic acid and 100 mcg of vitamin B12 for two years significantly improved measures of immediate and delayed memory and slowed the rise in plasma homocysteine concentrations (57). However, supplemented subjects had no reduction in homocysteine concentrations compared to baseline, nor did they perform better in processing speed tests compared to placebo. Another two-year, randomized, placebo-controlled study in elderly adults reported that a daily regimen of 800 mcg of folic acid, 500 mcg of vitamin B12, and 20 mg of vitamin B6 significantly reduced the rate of brain atrophy compared to placebo treatment (0.5% vs. 3.7%). Interestingly, a greater benefit was seen in those with high compared to low homocysteine concentrations at baseline, suggesting the importance of lowering homocysteine levels in prevention of brain atrophy and cognitive decline (58, 59). The authors attributed the changes in homocysteine levels primarily to vitamin B12(59). Finally, the most recent randomized, double blind, placebo-controlled trial in over 2,500 individuals who suffered a stroke showed that the normalization of homocysteine concentrations by B-vitamin supplementation (2 mg of folic acid, 500 mcg of vitamin B12, and 25 mg of vitamin B6) did not improve cognitive performance or decrease incidence of cognitive decline compared to placebo (60). Currently, there is a need for larger trials to evaluate the effect of B-vitamin supplementation on long-term outcomes, such as the incidence of Alzheimer’s disease.
Observational studies have found as many as 30% of patients hospitalized for depression are deficient in vitamin B12 (61). A cross-sectional study of 700 community-living, physically disabled women over the age of 65 found that vitamin B12-deficient women were twice as likely to be severely depressed as non-deficient women (62). A population-based study in 3,884 elderly men and women with depressive disorders found that those with vitamin B12 deficiency were almost 70% more likely to experience depression than those with normal vitamin B12 status(63). The reasons for the relationship between vitamin B12 deficiency and depression are not clear but may involve a shortage in S-adenosylmethionine (SAM). SAM is a methyl group donor for numerous methylation reactions in the brain, including those involved in the metabolism of neurotransmitters whose deficiency has been related to depression (64). Severe vitamin B12 deficiency in a mouse model showed dramatic alterations in the level of DNA methylation in the brain, which might lead to neurologic impairments (65). This hypothesis is supported by several studies that have shown supplementation with SAM improves depressive symptoms (66-69).
Increased homocysteine level is another nonspecific biomarker of vitamin B12deficiency that has been linked to depressive symptoms in the elderly (70). However, in a recent cross-sectional study conducted in 1,677 older individuals, higher vitamin B12 plasma levels, but not changes in homocysteine concentrations, were correlated with a lower prevalence of depressive symptoms (71). Few studies have examined the relationship of vitamin B12 status, homocysteine levels, and the development of depression over time. In a randomized, placebo-controlled,intervention study with over 900 older participants experiencing psychological distress, daily supplementation with folic acid (400 mcg) and vitamin B12 (100 mcg) for two years did not reduce the occurrence of symptoms of depression despite significantly improving blood folate, vitamin B12, and homocysteine levels compared to placebo (72). However, in a long-term randomized, double-blind, placebo-controlled study among sufferers of cerebrovascular accidents at high risk of depression, daily supplementation with 2 mg of folic acid, 25 mg of vitamin B6, and 500 mcg vitamin B12 significantly lowered the risk of major depressive episodes during a seven-year follow-up period compared to placebo (73). Although it cannot yet be determined whether vitamin B12 deficiency plays a causal role in depression, it may be beneficial to screen for vitamin B12 deficiency in older individuals as part of a medical evaluation for depression.
High homocysteine levels may affect bone remodeling by increasing bone resorption(breakdown), decreasing bone formation, and reducing bone blood flow. Another proposed mechanism involves the binding of homocysteine to the collagenous matrix of bone, which may modify collagen properties and reduce bone strength (reviewed in 74). Alterations of bone biomechanical properties can contribute toosteoporosis and increase the risk of fractures in the elderly. Since vitamin B12 is a determinant of homocysteine metabolism, it was suggested that the risk of osteoporotic fractures in older subjects might be enhanced by vitamin B12deficiency. A meta-analysis of four observational studies, following a total of 7,475 older individuals for 3 to 16 years, found a weak association between an elevation in vitamin B12 of 50 picomoles/L in blood and a reduction in fracture risk (75). Arandomized, placebo-controlled trial in 559 elderly individuals with low serum levels of folate and vitamin B12 and at increased risk of fracture evaluated the combined supplementation of very high doses of folic acid (5 mg/day) and vitamin B12 (1.5 mg/day). The two-year study found that the supplementation improved B-vitamin status, decreased homocysteine concentrations, and reduced risk of total fractures compared to placebo (76). However, a multicenter study in 5,485 subjects withcardiovascular disease or diabetes mellitus showed that daily supplementation with folic acid (2.5 mg), vitamin B12 (1 mg), and vitamin B6 (50 mg) lowered homocysteine concentrations but had no effect on fracture risk compared to placebo(77). Another small, randomized, double-blind trial in 93 individuals with low vitamin D status found no additional benefit of B-vitamin supplementation (50 mg/day of vitamin B6, 0.5 mg/day of folic acid, and 0.5 mg/day of vitamin B12) on markers of bone health over a one-year period beyond that associated with vitamin D and calcium supplementation. Yet, the short-scale of the study did not permit a conclusion on whether the lowering of homocysteine through B-vitamin supplementation could have long-term benefits on bone strength and fracture risk(78). A large intervention study conducted in older people with no preexisting conditions is under way to evaluate the effect of B-vitamin supplementation on markers of bone health and incidence of fracture; this trial might clarify whether B vitamins could have a protective effect on bone health in the elderly population(79).
Food sources
Only bacteria can synthesize vitamin B12 (80). Vitamin B12 is present in animal products, such as meat, poultry, fish (including shellfish), and to a lesser extent dairy products and eggs (1). Fresh pasteurized milk contains 0.9 mcg per cup and is an important source of vitamin B12 for some vegetarians (17). Those strict vegetarians who eat no animal products (vegans) need supplemental vitamin B12 to meet their requirements. Recent analyses revealed that some plant-source foods, such as certain fermented beans and vegetables and edible algae and mushrooms, contain substantial amounts of bioactive vitamin B12 (81). Together with B-vitaminfortified food and supplements, these foods may constitute new alternatives to prevent vitamin B12 deficiency in individuals consuming vegetarian diets. Also, individuals over the age of 50 should obtain their vitamin B12 in supplements or fortified foods (e.g., fortified cereals) because of the increased likelihood of food-bound vitamin B12 malabsorption with increasing age.
Most people do not have a problem obtaining the RDA of 2.4 mcg/day of vitamin B12in food. According to a US national survey, the average dietary intake of vitamin B12 is 5.4 mcg/day for adult men and 3.4 mcg/day for adult women. Adults over the age of 60 had an average dietary intake of 4.8 mcg/day (42). However, consumption of any type of vegetarian diet dramatically increases the prevalence of vitamin B12 deficiency in individuals across all age groups (82). Some foods with substantial amounts of vitamin B12 are listed in the table below along with their vitamin B12 content in micrograms (mcg). For more information on the nutrient content of specific foods, search the USDA food composition database.
| Food | Serving | Vitamin B12 (mcg) |
| Clams (steamed) | 3 ounces | 84.1 |
| Mussels (steamed) | 3 ounces | 20.4 |
| Mackerel (Atlantic, cooked, dry-heat) | 3 ounces* | 16.1 |
| Crab (Alaska king, steamed) | 3 ounces | 9.8 |
| Beef (lean, plate steak, cooked, grilled) | 3 ounces | 6.9 |
| Salmon (chinook, cooked, dry-heat) | 3 ounces | 2.4 |
| Rockfish (cooked, dry-heat) | 3 ounces | 1.0 |
| Milk (skim) | 8 ounces | 0.9 |
| Turkey (cooked, roasted) | 3 ounces | 0.8 |
| Brie (cheese) | 1 ounce | 0.5 |
| Egg (poached) | 1 large | 0.4 |
| Chicken (light meat, cooked, roasted) | 3 ounces | 0.3 |
*A three-ounce serving of meat or fish is about the size of a deck of cards.
Cyanocobalamin is the principal form of vitamin B12 used in oral supplements, but methylcobalamin is also available as a supplement. Cyanocobalamin is available by prescription in an injectable form and as a nasal gel for the treatment of pernicious anemia. Over-the-counter preparations containing cyanocobalamin include multivitamins, vitamin B-complex supplements, and single-nutrient, vitamin B12supplements (83).
Toxicity
No toxic or adverse effects have been associated with large intakes of vitamin B12from food or supplements in healthy people. Doses as high as 2 mg (2,000 mcg) daily by mouth or 1 mg monthly by intramuscular (IM) injection have been used to treat pernicious anemia without significant side effects (84). When high doses of vitamin B12 are given orally, only a small percentage can be absorbed, which may explain the low toxicity (4). Because of the low toxicity of vitamin B12, no tolerable upper intake level (UL) has been set by the US Food and Nutrition Board (17).
A number of drugs reduce the absorption of vitamin B12. Proton-pump inhibitors (e.g., omeprazole and lansoprazole), used for therapy of Zollinger-Ellison syndromeand gastroesophageal reflux disease (GERD), markedly decrease stomach acid secretion required for the release of vitamin B12 from food but not fromsupplements. Long-term use of proton-pump inhibitors has been found to decrease blood vitamin B12 levels. However, vitamin B12 deficiency does not generally develop until after at least three years of continuous therapy (85, 86). Another class of gastric acid inhibitors known as Histamine2 (H2)-receptor antagonists (e.g., cimetidine, famotidine, and ranitidine), often used to treat peptic ulcer disease, has also been found to decrease the absorption of vitamin B12 from food. It is not clear whether the long-term use of H2-receptor antagonists could cause overt vitamin B12 deficiency (87, 88). Individuals taking drugs that inhibit gastric acid secretion should consider taking vitamin B12 in the form of a supplement because gastric acid is not required for its absorption. Other drugs found to inhibit vitamin B12 absorption from food include cholestyramine (a bile acid-binding resin used in the treatment of high cholesterol), chloramphenicol and neomycin (antibiotics), and colchicine (medicine for gout treatment). Metformin, a medication for individuals with type 2diabetes, was found to decrease vitamin B12 absorption by tying up free calcium required for absorption of the IF-B12 complex (89). However, the clinical significance of this is unclear (90). It is not known whether calcium supplementation can reverse vitamin B12 malabsorption; therefore, calcium supplementation is not currently prescribed for the prevention or treatment of metformin-induced vitamin B12deficiency (91). Previous reports that megadoses of vitamin C destroy vitamin B12have not been supported (92) and may have been an artifact of the assay used to measure vitamin B12 levels (17).
Nitrous oxide, a commonly used anesthetic, oxidizes and inactivates vitamin B12, thus inhibiting both of the vitamin B12-dependent enzymes, and can produce many of the clinical features of vitamin B12 deficiency, such as megaloblastic anemia orneuropathy. Since nitrous oxide is commonly used for surgery in the elderly, some experts feel vitamin B12 deficiency should be ruled out prior to its use (6, 15).
Large doses of folic acid given to an individual with an undiagnosed vitamin B12deficiency could correct megaloblastic anemia without correcting the underlying vitamin B12 deficiency, leaving the individual at risk of developing irreversibleneurologic damage (17). For this reason, the Food and Nutrition Board of the US Institute of Medicine advises that all adults limit their intake of folic acid (supplements and fortification) to 1,000 mcg (1 mg) daily.
Linus Pauling Institute Recommendation
A varied diet should provide enough vitamin B12 to prevent deficiency in most individuals 50 years of age and younger. Strict vegetarians and women planning to become pregnant should take a multivitamin supplement daily or eat fortifiedcereal, which would ensure a daily intake of 6 to 30 mcg of vitamin B12 in a form that is easily absorbed. Higher doses of vitamin B12 supplements are recommended for patients taking medications that interfere with its absorption (see Drug interactions).
Older adults (> 50 years)
Because vitamin B12 malabsorption and vitamin B12 deficiency are more common in older adults, the Linus Pauling Institute recommends that adults older than 50 years take 100 to 400 mcg/day of supplemental vitamin B12.
http://lpi.oregonstate.edu/infocenter/vitamins/vitaminB12/#food_source
Written in March 2003 by:
Jane Higdon, Ph.D.
Linus Pauling Institute
Oregon State University
Updated in January 2014 by:
Barbara Delage, Ph.D.
Linus Pauling Institute
Oregon State University
Reviewed in April 2014 by:
Joshua W. Miller, Ph.D.
Professor and Chair, Department of Nutritional Sciences
Rutgers, The State University of New Jersey
Copyright 2000-2014 Linus Pauling Institute
Disclaimer
The Linus Pauling Institute Micronutrient Information Center provides scientific information on the health aspects of dietary factors and supplements, foods, and beverages for the general public. The information is made available with the understanding that the author and publisher are not providing medical, psychological, or nutritional counseling services on this site. The information should not be used in place of a consultation with a competent health care or nutrition professional.
The information on dietary factors and supplements, foods, and beverages contained on this Web site does not cover all possible uses, actions, precautions, side effects, and interactions. It is not intended as nutritional or medical advice for individual problems. Liability for individual actions or omissions based upon the contents of this site is expressly disclaimed.

Foods highest in antioxidants
[hide]
In the following discussion, the term “antioxidant” refers mainly to non-nutrient compounds in foods, such as polyphenols, which haveantioxidant capacity in vitro and so provide an artificial index of antioxidant strength – the ORAC measurement. Other than for dietary antioxidant vitamins – vitamin A, vitamin C and vitamin E – no food compounds have been proved with antioxidant efficacy in vivo. Accordingly, regulatory agencies like the Food and Drug Administration of the United States and the European Food Safety Authority(EFSA) have published guidance disallowing food product labels to claim an inferred antioxidant benefit when no such physiological evidence exists.[1][2]
Many common foods contain rich sources of polyphenols which have antioxidant properties only in test tube studies. As interpreted by theLinus Pauling Institute, dietary polyphenols have little or no direct antioxidant food value following digestion.[3] Not like controlled test tube conditions, the fate of flavones or polyphenols in vivo shows they are poorly conserved (less than 5%), with most of what is absorbed existing as metabolites modified during digestion and destined for rapid excretion.[4]
Spices, herbs, and essential oils are rich in polyphenols in the plant itself and shown with antioxidant potential in vitro. Typical spices high in polyphenols (confirmed in vitro) are clove, cinnamon, oregano, turmeric, cumin, parsley, basil, curry powder, mustard seed, ginger,pepper, chili powder, paprika, garlic, coriander, onion and cardamom. Typical herbs are sage, thyme, marjoram, tarragon, peppermint,oregano, savory, basil and dill weed.
Dried fruits are a good source of polyphenols by weight/serving size as the water has been removed making the ratio of polyphenols higher. Typical dried fruits are pears, apples, plums, peaches, raisins, figs and dates. Dried raisins are high in polyphenol count. Red wine is high in total polyphenol count which supplies antioxidant quality which is unlikely to be conserved following digestion (see section below).
Deeply pigmented fruits like cranberries, blueberries, plums, blackberries, raspberries, strawberries, blackcurrants, figs, cherries, guava, oranges, mango, grape juice and pomegranate juice also have significant polyphenol content.
Typical cooked vegetables rich in antioxidants are artichokes, cabbage, broccoli, asparagus, avocados, beetroot and spinach.
Nuts are a moderate source of polyphenol antioxidants. Typical nuts are pecans, walnuts, hazelnuts, pistachio, almonds, cashew nuts,macadamia nuts and peanut butter.
Sorghum bran, cocoa powder, and cinnamon are rich sources of procyanidins, which are large molecular weight compounds found in many fruits and some vegetables. Partly due to the large molecular weight (size) of these compounds, their amount actually absorbed in the body is low, an effect also resulting from the action of stomach acids, enzymes and bacteria in the gastrointestinal tract where smaller derivatives are metabolized and prepared for rapid excretion.[3][4]
Despite the above discussion implying that ORAC-rich foods with polyphenols may provide antioxidant benefits when in the diet, there remains no physiological evidence that any polyphenols have such actions or that ORAC has any relevance in the human body.
On the contrary, research indicates that although polyphenols are good antioxidants in vitro, antioxidant effects in vivo are probably negligible or absent.[5][6][7] By non-antioxidant mechanisms still undefined, polyphenols may affect mechanisms of cardiovascular disease or cancer.[8]
The increase in antioxidant capacity of blood seen after the consumption of polyphenol-rich (ORAC-rich) foods is not caused directly by the polyphenols, but most likely results from increased uric acid levels derived from metabolism of flavonoids.[3][4] According to Frei, “we can now follow the activity of flavonoids in the body, and one thing that is clear is that the body sees them as foreign compounds and is trying to get rid of them.”[4] Another mechanism may be the increase in activities of paraoxonases by dietary antioxidants which can reduce oxidative stress.[9]
Natural phenols are a class of molecules found in abundance in plants.
Flavonoids, a subset of polyphenol antioxidants, are present in many berries, as well as in coffee and tea.
While there is ample evidence to indicate the health benefits of diets rich in fruits, vegetables, legumes, whole grains and nuts, no specific food has been acknowledged by scientists and government regulatory authorities as providing a health benefit. Current medical research is focused on whether health effects could be due to specific essential nutrients or phytochemicals.[1]
The following is a list of phytochemicals present in commonly consumed foods.
[hide]
orange pigments
yellow pigments.
A phytoestrogens – seeds (flax, sesame, pumpkin, sunflower, poppy), whole grains (rye, oats, barley), bran (wheat, oat, rye), fruits (particularly berries) and vegetables.[2]
wholegrain wheat, rye and barley
Other common name(s): certain phytochemicals may be called antioxidants, flavonoids, flavanols, flavanones, isoflavones, catechins, epicatechins, anthocyanins, anthocyanidins, proanthocyanidins, isothiocyanates, carotenoids, allyl sulfides, polyphenols, phenolic acids, and many other names
Scientific/medical name(s): various names
The term “phytochemicals” refers to a wide variety of compounds made by plants, but is mainly used to describe those compounds that may affect human health. Phytochemicals are found in plant-based foods such as fruits, vegetables, beans, and grains. Scientists have identified thousands of phytochemicals, although only a small fraction have been studied closely. Some of the better-known phytochemicals include beta carotene and other carotenoids, ascorbic acid (vitamin C), folic acid, and vitamin E.
Some phytochemicals have either antioxidant or hormone-like actions. There is some evidence that a diet rich in fruits, vegetables, and whole grains reduces the risk of certain types of cancer and other diseases. Researchers are looking for specific compounds in these foods that may account for these healthful effects in humans. Available scientific evidence does not support claims that taking phytochemical supplements is as good for long-term health as consuming the fruits, vegetables, beans, and grains from which they are taken.
Phytochemicals are promoted for the prevention and treatment of many health conditions, including cancer, heart disease, diabetes, and high blood pressure. There is some evidence that certain phytochemicals may help prevent the formation of potential carcinogens (substances that cause cancer), block the action of carcinogens on their target organs or tissue, or act on cells to suppress cancer development. Many experts suggest that people can reduce their risk of cancer significantly by eating more fruits, vegetables, and other foods from plants that contain phytochemicals.
There are several major groups of phytochemicals.
The polyphenols include a large subgroup of chemicals called flavonoids. Flavonoids are plant chemicals found in a broad range of fruits, grains, and vegetables. They are being studied to find out whether they can prevent chronic diseases such as cancer and heart disease. The isoflavones found in foods and supplements such as soy products, red clover, garbanzo beans, and licorice and the lignans found in flaxseed and whole grains might mimic the actions of the female hormone estrogen (see Licorice and Soybean). These seemingly estrogen-like substances from these plant sources are called phytoestrogens. They may play a role in the development of and protection against some hormone-dependent cancers such as some types of breast and prostate cancer.
Other polyphenols (including some flavonoids) act as antioxidants. These are thought to rid the body of harmful molecules known as free radicals, which can damage a cell’s DNA and may trigger some forms of cancer and other diseases. These compounds are commonly found in teas and in vegetables such as broccoli, Brussels sprouts, cabbage, and cauliflower. Grapes, eggplant, red cabbage, and radishes all contain anthocyanidins — flavonoids that are thought to act as antioxidants and may protect against some cancers and heart disease. Quercetin, another flavonoid that appears to have antioxidant properties, is found in apples, onions, teas, and red wine. Ellagic acid, found in raspberries, blackberries, cranberries, strawberries, and walnuts, is being studied to see if it has anti-cancer effects (see Ellagic Acid).
Carotenoids, which give carrots, yams, cantaloupe, butternut squash, and apricots their orange color, are promoted as anti-cancer agents (see Vitamin A, Retinoids, and Provitamin A Carotenoids). Tomatoes, red peppers, and pink grapefruit contain lycopene, which proponents claim is a powerful antioxidant (see Lycopene). The phytochemicals lutein and zeaxanthin are carotenoids found in spinach, kale, and turnip greens that may reduce the risk of some cancers.
Another group of phytochemicals, called allyl sulfides, are found in garlic and onions (see Garlic). These compounds may stimulate enzymes that help the body get rid of harmful chemicals. They may also help strengthen the immune system.
Phytochemicals are present in virtually all of the fruits, vegetables, legumes (beans and peas), and grains we eat, so it is quite easy for most people to include them in their diet. For instance, a carrot contains more than a hundred phytochemicals. There are thousands of known phytochemicals, but only a few have been studied in detail.
Many of the better-known phytochemicals can be purchased as dietary supplements. However, most available evidence suggests that these single supplements are not as good for you as the foods from which they are derived.
Only a few years ago, the term “phytochemical” was barely known. But doctors, nutritionists, and other health care practitioners have long advocated a low-fat diet that includes a variety of fruits, vegetables, legumes, and whole grains. Historically, cultures that consume such a diet have lower rates of certain cancers and heart disease.
Since the passage of the Dietary Supplement Health and Education Act (DSHEA) in the United States in 1994, a growing number of phytochemicals are being sold as dietary supplements.
The idea that a diet rich in fruits, vegetables, legumes, and grains reduces the risk of cancer, heart disease, and other illnesses is widely accepted. But only recently have researchers begun to try to learn the effects of specific phytochemicals contained in those foods.
Because of the number of phytochemicals and the complexity of the chemical processes in which they are involved, it is difficult for researchers to find out which phytochemicals in foods may fight cancer and other diseases, which may have no effect, and which may even be harmful.
Much of the evidence so far has come from observations of cultures in which the diet comes mainly from plant sources, and which seem to have lower rates of certain types of cancer and heart disease. For instance, the relatively low rates of breast and endometrial cancers in some Asian cultures are credited at least in part to dietary habits. These cancers are much more common in the United States, possibly because the typical American diet is higher in fat and lower in fruits, vegetables, legumes, and grains. Part of the lower risk in Asian cultures is likely due to other factors such as lower obesity rates and more exercise.
Many studies have looked at the relationship between cancer risk and eating fruits and vegetables, legumes, and whole grains. Most of the evidence indicates that eating a diet high in these foods seems to lower the risk of some cancers and other illnesses.
Some of the links between individual phytochemicals and cancer risk found in laboratory studies are compelling and make a strong case for further research. So far, however, none of the findings are conclusive. It is still uncertain which of the many phytochemicals in fruits and vegetables actively helps the body fight disease.
Researchers have also shown much interest in phytochemical supplements. Some laboratory studies in cell cultures and animals have shown that certain phytochemicals have some activity against cancer cells or tumors. But at this time there have been no strong studies in humans showing that any phytochemical supplement can prevent or treat cancer.
Until conclusive research findings emerge, the American Cancer Society’s 2012 nutrition guidelines recommend choosing what you eat and drink in amounts that help you get to and stay at a healthy weight. Eating a balanced diet that includes 2½ cups of vegetables and fruits each day and choosing whole grains over refined grains and sugar-sweetened products should be part of this plan. Limiting intake of red meats and processed meats such as bacon, sausage, lunch meats, and hot dogs is also recommended in order to help reduce cancer risk. A good way to do this is to choose fish, poultry, or beans for some meals rather than beef, pork, lamb, or processed meats. The guidelines note that although eating fish is linked to a lower risk of heart disease, the evidence regarding cancer in humans is limited. A balanced diet with foods from a variety of plant sources is likely to be more effective in reducing cancer risk than consuming large amounts of a few phytochemicals.
Phytochemicals, in the amounts consumed in a healthy diet, are likely to be helpful and are unlikely to cause any major problems. Some people assume that because phytochemical supplements come from “natural” sources, they must be safe and free from side effects, but this is not always true. Many phytochemical supplements, especially when taken in large amounts, have side effects and may interact with some drugs. Some of these interactions may be dangerous. Before taking a phytochemical in supplement form, consider talking to your doctor and pharmacist to be sure it will not interact with other medicines or herbs you may be taking. Relying on the use of phytochemicals alone and avoiding or delaying conventional medical care for cancer may have serious health consequences

This is a very popular question. And an important one, but even if you aren’t following a plant-based diet, do YU know how much protein you should be eating on a daily basis?
How much protein do we actually need?
Well, in the United States, the Dietary Reference Intake (DRI) for protein is 0.8 to 1.0 grams of protein per kilogram of body weight. To calculate your weight in kilograms, divide your weight in pounds by 2.2. That number is about how many grams you need each day. Approximately 15-25% of your total calories should be from protein sources. Although protein is certainly an essential nutrient, which plays many key roles in the way our bodies function, we do not need huge quantities of it.
Many Americans consume about twice the amount of protein necessary, and it’s important to note that excess protein can’t be stored in the body—ultimately, its elimination strains the liver and kidneys. Excessive protein consumption is linked to certain cancers (i.e.: colon, breast, prostate, pancreas), kidney disease and even osteoporosis. If you’re consuming a variety of clean, whole foods, you should get all the protein you need, without taxing your body.
Like this article so far? Share it with others on Twitter by clicking here.
Why is protein so important?
As you may or may not know, proteins are made up of amino acids, and they are the “building blocks” of life. Our skin, muscles, tendons, cartilage, even hair and nails, are all thanks to protein. Protein helps form enzymes, hormones, antibodies and new tissues. It replaces old cells with shiny new ones, and it transports important nutrients in and out of those cells. The human body can manufacture all but nine of the 22 amino acids that make up proteins. These nine amino acids are known as “essential” amino acids, and therefore must be derived from what we eat. There’s a lot of overlap from the sources of these “essentials,” which further proves that variety is best for covering bases. You don’t have to sweat every detail, or spend a ton of time planning meals—eat an assortment of whole foods and you will get what you need.
* Arginine
Classified as a semi-essential or “conditionally” essential amino acid, depending on the developmental stage and health status of the individual.
Find it in: almonds, beets, Brazil nuts, buckwheat, carrots, cashews, celery, chickpeas, coconut, cucumbers, flax seed, garlic, green vegetables, hazelnuts, kidney beans, leeks, lentil, lettuce, nutritional yeast, onion, parsnips, pecans, pine nuts, potatoes, pumpkin seeds, radishes, sesame seeds, sprouts, sunflower seeds and walnuts.
. . .
Histidine
Especially needed during infancy for proper growth and development—once was believed to be only essential for newborns, but is now known to be essential for adults, as well.
Find it in: apples, bananas, beans, beets, buckwheat, carrots, cantaloupe, cauliflower, celery, citrus fruits, cucumber, dandelion, endive, garlic, greens, legumes, mushrooms, pomegranates, radish, rice, seaweed, sesame, spinach, spirulina and turnip greens.
. . .
Isoleucine
Necessary for muscle production, maintenance and recovery—especially post-workout. Involved in hemoglobin formation, regulating blood sugar levels, blood clot formation and energy.
Find it in: almonds, avocados, cashews, chickpeas, coconut, lentils, olives, papaya, seaweed and most seeds like sunflower.
. . .
Leucine
Essential for growth hormone production, tissue production and repair. Prevents muscle wasting and is used in treating conditions such as Parkinson’s disease.
Find it in: almonds, asparagus, avocados, chickpeas, coconut, lentils, oats, olives, papayas, rice, sunflower seeds and walnuts.
. . .
Lysine
Great for calcium absorption, bone development, nitrogen maintenance, tissue repair, hormone production, antibody production.
Find it in: amaranth, apples, apricots, beans, beets, carrots, celery, cucumber, dandelion greens, grapes, papayas, parsley, pears, peas, spinach and turnip greens.
. . .
Methionine
The “cleaner”—important for fat emulsification, digestion, antioxidant (cancer prevention), arterial plaque prevention (heart health) and heavy metal removal.
Find it in: black beans, Brazil nuts, cashews, kidney beans, oats, sesame seeds, spirulina, spinach, sunflower seeds and watercress.
. . .
Phenylalanine
A precursor for tyrosine and the signaling molecules: dopamine, norepinephrine (noradrenaline) and epinephrine (adrenaline), as well as the skin pigment: melanin. Supports learning and memory, brain processes and mood elevation.
Find it in: apples, beets, carrots, cashews, flax seed, hazelnuts, nutritional yeast, parsley, pineapples, pumpkin seeds, sesame seeds, sunflower seeds, spinach and tomatoes.
. . .
Threonine
Monitors bodily proteins for maintaining or recycling processes.
Find it in: almonds, beans, carrots, celery, chickpeas, collards, flax seed, greens, green leafy vegetables, kale, lentils, lima beans, nori, nuts, papayas, sesame seeds, sunflower seeds and walnuts.
. . .
Tryptophan
Needed for niacin production, serotonin production, pain management, sleep and mood regulation.
Find it in: Brussels sprouts, carrots, celery, chives, dandelion greens, endive, fennel, nutritional yeast, pumpkin seeds, sesame seeds, snap beans, spinach, sunflower seeds, turnips and walnuts.
. . .
Valine
Helps muscle production, recovery, energy, endurance—balances nitrogen levels and is used in treatment of alcohol-related brain damage.
Find it in: apples, almonds, bananas, beets, broccoli, carrots, celery, dandelion greens, lettuce, nutritional yeast, okra, parsley, parsnips, pomegranates, potatoes, squash, tomatoes and turnips.
You may need more protein if you are…
• Mentally/physically tired (especially if you need daytime naps)
• Suffering from injuries/cramping/muscle soreness
• Unable to concentrate or focus
• Losing muscle, or unable to build it
• Losing hair
• Suffering from brittle/breaking nails
• Unusually susceptible to sunburn
• Suffering from headaches, fainting, nausea
• Cranky, anxious or moody or depressed
Remember, our bodies are designed, and biologically programmed, to survive. Symptoms are the way your body tries to communicate with you. If it doesn’t have enough of what it needs to thrive, it will do its best to get what it needs with what it has. If you are unable to build/retain muscle, that’s probably because you aren’t getting enough protein and your body is taking it from where it can—your muscle tissue. If you suffer from recurring/multiple injuries, your body probably doesn’t have the protein it needs for strength, rebuilding and recovery. Are your nails flimsy and breaking? Are you losing excessive hair? Your body may be holding onto what protein it has stored in the “bank,” versus using what little it has to create new nails or full hair.
This is also why nutrient-rich, whole foods are ideal, and why true health comes from these kinds of foods versus labels like “vegan.” Just because someone is vegan, vegetarian, or an omnivore for that matter, doesn’t make them healthy. Many folks make the mistake of “going vegan” and consuming a lot of processed, nutrient-void junk foods, pastas, etc. True health comes from the consumption of a variety of whole foods—the ones Mother Nature designed. It’s that simple.
Want to see how delicious plant-powerful recipes can be?

And here’s a helpful chart.
This chart is for reference only, since it’s recommended that you think of food in its “wholeness”—its natural, plant-based complexity. Excellent nutrition is truly about balance and variety. For example, everything that makes up a carrot is important for good health, not just the beta carotene, or the vitamin C, but the whole carrot. It’s packaged how Mother Nature designed—a symphony of nutrients, fiber and a large assortment of protective compounds, most of which still remain unnamed (and undiscovered). Imagine that.

Do I need to combine protein sources at each meal to make sure I get all essential amino acids?
No. It’s a myth. Nearly all whole foods (including greens and veggies) contain protein, and nearly all forms of protein contain all protein-forming amino acids in some quantity. If you eat a variety of nutrient-rich, whole foods, your body will work its magic to store what it needs to function optimally. Scientists used to claim that herbivores would develop protein deficiency if they didn’t get essential amino acids in proper, combined amounts at every meal. But our bodies are amazing. See, when we eat, amino acid “deposits” are made into a “storage bank,” and the body then takes what it needs as it’s needed. So, you don’t have to eat complementary proteins together with each meal in an effort to make complete protein. Your body has a system already set up; you just need to eat a variety of foods to fill the bank. By eating a variety of plant foods with “incomplete proteins” throughout the day, we can easily get enough “complete protein.”
Picture a giant 400lb gorilla. What does he eat to grow that strong, muscular body? Leaves, stems, roots, seeds and fruit (and maybe the occasional insect that lives on those foods). The body actually works less (uses less energy) to process protein from a vegetable-based diet than it does from a meat-based diet, too. This energy conservation is great for more efficient healing, building and overall optimal health. Most plant-based protein sources, contrary to animal-based sources, are also alkalizing for the body. Which means less aches and pains, freedom from disease, better sleep, happier moods, improved memory and concentration, stronger/more efficient digestion and an overall better state of health.
Complete Plant Protein Sources
Remember—variety. And if you want to make it even easier for yourself, here are a bunch of delicious, whole food options for complete plant-based proteins that you can keep in your pantry and fridge. Add them to salads, smoothies, wraps and more.
It’s also helpful to have a plant-based protein smoothie like Vega One once a day. It contains 15 grams of quality plant-based protein per serving (enter SHIPUSVEGA at checkout to get free shipping)—I usually have one a day with two scoops.
(These are gluten-free, too)
Amaranth: recipes | how to pop
Spirulina & Chlorella: add to smoothies, or take in powder or tablets
Buckwheat: recipes | how to cook
Chia Seed: recipes
Hemp Seed: hemp milk recipe
Quinoa: cooking tips and recipes
Sprouted Lentils (sprouting makes them complete):
how to sprout lentils | lentil recipes
***
Print out this helpful Plant Protein Chart and keep it in your wallet or purse. Use it as a reference when planning meals for the week, or when shopping.
***
It’s all about variety.
While the protein question is a frequent one for plant-based eaters, don’t dismiss it in an uneducated haze of herbivore pride. It’s very important that we get enough protein each and every day, but as you can see, it’s not as difficult as most folks think—it’s actually quite easy (and did we mention delicious?). Variety is the key to acquiring all of the essential amino acids that we need, and YumUniverse shares an infinite collection of clean, whole food recipes that include this variety. Truly a universe of possibilities. Have fun with it.


