The lifespan extension associated with dietary restriction may be due less to a reduction in calories, and more to a reduction in animal protein (particularly the amino acid leucine, which may accelerate aging via the enzyme TOR).
Category: Articles
Ten servings of fruit and vegetables a day — not five — needed for good health, researchers say
 Sarah Knapton, The Daily Telegraph, National Post Wire Services | April 1, 2014 | Last Updated: Apr 1 10:06 AM ET
Sarah Knapton, The Daily Telegraph, National Post Wire Services | April 1, 2014 | Last Updated: Apr 1 10:06 AM ETMore from National Post Wire Services

FotoliaFive a day won’t cut it: Researchers now say 10 servings of fruit and veg are needed per day for optimum health.
A healthy diet should include 10 portions of fruit and vegetables a day, doubling the five-a-day official advice, say British health experts.
The research, which involved a 12-year study, also found that vegetables were four times healthier than fruit.
The study, by University College London, found that eating large quantities of fruit and vegetables significantly lowered the risk of premature death. People who ate at least seven portions of fruit and vegetables each day were 42%less likely to die from any cause over the course of the study.
Prof Simon Capewell, of the department of public health at the University of Liverpool, said the advice should be 10 portions a day. “Humans are designed to be omnivorous: a handful of nuts, seeds, fruit and the occasional antelope. We’re not meant to be eating junk food.”
Researchers examined the eating habits of 65,000 people in England between 2001 and 2013.
They found that seven helpings a day of fruit or vegetables could reduce a person’s overall risk of premature death by 42% when compared with people who ate just one whole portion.
People who ate between five and seven portions a day had a 36% reduced risk of death, those who ate three to five portions had a 29% decreased risk and those who ate one to three helpings had a 14% reduced risk.
Those with the highest intakes were also 25% less likely to die from cancer and 31% less likely to die from heart disease.
To implement a seven-a-day message would be really challenging for many in society and would require governmental support
“We need to urgently examine seriously the proposal to increase recommended intake to seven a day,” said Naveed Sattar, professor of metabolic medicine at the University of Glasgow. “To implement a seven-a-day message would be really challenging for many in society and would require governmental support such as subsidising the cost of fruitand vegetables, perhaps by taxing sugar-rich foods.”
The study also found that vegetables were far more beneficial than fruit. Each portion of vegetables lowered the risk of death by 16 per cent. However, each piece of fruit only lowered the chance of death by 4 per cent.
The authors said the findings lent support to the Australian government’s advice of “two plus five” a day, which encourages people to eat two helpings of fruit and five of vegetables. Dr Alison Tedstone, the group’s director of diet and obesity, said: “Our focus remains on increasing overall consumption of fruit and vegetables to meet current recommendations.”
The study was published in the Journal of Epidemiology and Community Health.
Starving Tumors of Their Blood Supply

About a third of common cancers may be prevented by eating a healthy, plant-based diet; being physically active; and maintaining a healthy weight. One of the ways plants may help is by cutting off the supply lines to cancerous tumors.
A tumor cannot grow without a blood supply. Currently, it is believed that a tumor mass cannot exist in a volume greater than about the size of the ball at the tip of a ballpoint pen without a proper blood supply. This indicates that angiogenesis, the creation of new blood vessels, is critical to tumor growth.
Each one of us has cancer cells in us right now. One study describes how “by age 70, microscopic cancers are detected in the thyroid glands of virtually everyone. Most of these tumors never cause problems or become clinically significant, leading to the concept of ‘cancer without disease’ as a normal state during aging.” Cancer cells are commonly present in the body, but they can’t grow into tumors any bigger than that tiny dot size–no more than 10 million cancer cells–before needing to get hooked up to a blood supply. One way cancer turns on the tap is silencing certain tumor suppressor genes. How do we turn them back on? See, for example, Apple Skin: Peeling Back Cancer.
Another way tumors commandeer a blood supply is by diabolically releasing angiogenic factors, chemicals that cause new blood vessels to sprout into the tumor. The most important one is called vascular endothelial growth factor (VEGF). But we may be able to suppress VEGF with veggies.
Many of the phytonutrients we know and love in tea, spices, fruit, berries, broccoli, and beans can block cancer’s stimulation of new blood vessels. They’re ideal for prophylactic long-term use against breast cancer because of their reliability, availability, safety, and affordable price. A recent review concluded that we now have “convincing evidence that dietary plant constituents possess the unique ability to affect tumor angiogenesis, which may be deemed advantageous in the prevention and treatment of human breast cancer and other tumors.”
Most of these studies have only been done in a petri dish, though. Researchers stimulate human blood vessel cells and they start forming tubular structures trying to make new capillaries to feed the tumor. This tube formation can be substantially blocked by adding add plant compounds such as apigen or luteolin, found throughout the plant kingdom in foods such as citrus, celery, and peppers. In a study outlined in my video, Anti-Angiogensis: Cutting Off Tumor Supply Lines, you can see the effect of fisitin, a phytonutrient found in strawberries, shrinking the beginnings of new blood vessel formation. How else can strawberries smack on the cancer kibosh? See Strawberries versus Esophageal Cancer and Cancer Fighting Berries
Is porridge a miracle food?
Eating a regular bowl of oatmeal may mean cleaner arteries, protection from cancer
 Laura Donnelly, The Daily Telegraph, National Post Wire Services | March 19, 2014 | Last Updated: Mar 19 1:07 PM ET
Laura Donnelly, The Daily Telegraph, National Post Wire Services | March 19, 2014 | Last Updated: Mar 19 1:07 PM ETMore from National Post Wire Services

National Post filesGood, ol’ fashioned rolled oats could have some amazing benefits for your health, new studies suggest, reducing the likelihood of heart disease and some cancers.
Fans of porridge have long claimed that it gives them the best start to the day — but scientists say there is evidence that it could also have a special ingredient that actively cleans the arteries, protecting against cancer and heart disease.
A meeting of researchers says there is growing evidence that a bioactive compound contained only in oats may possess protective antioxidant properties.
Oats are the breakfast of choice for many athletes and dieters, who find the high fibre levels give them energy for longer. The combination of fibre, vitamins and minerals in whole grains has also been linked to a reduced risk of diseases. One particular fibre found only in oats — called beta-glucan — has already been credited with lowering cholesterol which can help protect against heart disease.
But scientists at the Annual Conference of the American Chemical Society in Dallas, Tex., yesterday said there was growing evidence that the benefits of oats do not just come from the fibre.
Researchers said studies suggested that a bioactive compound called avenanthramide could stop fat forming in the arteries, causing heart attacks and strokes.
Dr. Shengmin Sang, from the North Carolina Agricultural and Technical State University said: “While the data to support the importance of oat beta-glucan remains, these studies reveal that the heart health benefit of eating oats may go beyond fibre. As the scientific investigators dig deeper, we have discovered that the bioactive compounds found in oats may provide additional cardio-protective benefits.”
Fat formation in the arteries can become a condition called atherosclerosis in which the arteries become clogged with fatty substances such as cholesterol. This can lead to organ damage or blood clots that result in heart attacks or strokes.
Previous studies have suggested that the fibre contained in porridge can reduce cholesterol levels by as much as 23%. Studies on children have suggested the traditional breakfast dish can help to keep obesity at bay. Youngsters who eat oats regularly are 50% less likely to be overweight, one study of 10,000 children found.
Oats can reduce high blood pressure, which is closely linked to stroke and heart disease. They are also a source of vitamin B1, which is crucial for the nervous system
Oats can reduce high blood pressure, which is closely linked to stroke and heart disease. They are also a source of vitamin B1 (thiamin) which is crucial for the nervous system, and folic acid, which is essential for healthy fetal development. In an attempt to increase folic acid levels, pregnancy advisers have joined doctors in urging the Government to fortify flour with the acid to cut the number of babies developing defects such as spina bifida.
What is the “Real” Truth about Agave?
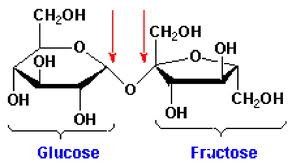
Fructose is the problem, agave is loaded with it.
If you knew the truth about what’s really in it, you’d be dumping it down the drain — and that would certainly be bad for sales.
Most agave “nectar” or agave “syrup” is nothing more than a laboratory-generated super-condensed fructose syrup, devoid of virtually all nutrient value, and offering you metabolic misfortune in its place.
Unfortunately, masterful marketing has resulted in the astronomical popularity of agave syrup among people who believe they are doing their health a favor by avoiding refined sugars like high fructose corn syrup, and dangerous artificial sweeteners.
And if you’re diabetic, you’ve been especially targeted and told this is simply the best thing for you since locally grown organic lettuce, that it’s “diabetic friendly,” has a “low glycemic index” and doesn’t spike your blood sugar.
While agave syrup does have a low-glycemic index, so does antifreeze — that doesn’t mean it’s good for you.
Most agave syrup has a higher fructose content than any commercial sweetener — ranging from 70 to 97 percent, depending on the brand, which is FAR HIGHER than high fructose corn syrup (HFCS), which averages 55 percent.
This makes agave actually WORSE than HFCS.
The Heme Iron Problem-Heme iron is the type of iron found in meat
Heme (blood) iron, cancer, and cardiovascular disease.
Iron encourages production of free radicals which can damage DNA and presumably increase cancer risk. In a study of over 14,000 individuals, high iron intake and high iron body stores were both positively linked to the risk of colon cancer. Higher levels of iron were associated with higher incidence of colon polyps, possible forerunners of colon tumors. However, cancer patients themselves had low levels of stored iron, indicating that cancer itself can deplete iron stores. [1]
Controversy has surrounded the question as to whether too much iron in your diet raises your risk for heart disease. A new study from the Harvard University School of Public Health brings new insight to the debate. Lasting for 4 years, this research involved more than 50,000 male health professionals. It was found that total iron intake was not associated with heart disease risk. But the source of the iron came was the principle factor. High levels of heme iron raised risk for heart disease twofold. Heme iron is the type of iron found in meat, chicken and fish.
Plant foods contain non-heme iron which appears to not be associated with risk for heart attack. Traditionally, many nutritionists used to consider non-heme iron to be inferior to the iron found in animal products, because non-heme iron is somewhat less well absorbed. But new evidence suggests that non-heme iron seems to be preferable.
When the body is low in iron, it can increase absorption of non-heme iron, and it can reduce adsorption when it already has sufficient amounts. The heme iron in meats tends to pass quickly right through the adsorption mechanism, thus entering the blood stream whether it is needed or not. Since vegetarians generally have adequate iron intake, it is clear that non-heme iron can easily meet nutritional needs. Also, plant iron doesn’t create the health risks of heme iron.
Iron increases heart disease risks because heme iron acts as a pro-oxidant, causing LDL-cholesterol — the ‘bad’ cholesterol — to react with oxygen. This reaction is involved in the formation of plaques in the arteries and therefore increases one’s risk of cardiovascular problems. The chart: http://www.ecologos.org/iron.htm
Avoiding Dairy to Prevent Parkinson’s
 There are four things that may reduce our risk of developing Parkinson’s disease: increase exercise, and avoid dairy products, pesticides, and head trauma (please wear your seatbelt and bike helmet!).
There are four things that may reduce our risk of developing Parkinson’s disease: increase exercise, and avoid dairy products, pesticides, and head trauma (please wear your seatbelt and bike helmet!).
What about avoiding pesticides and other industrial pollutants? A recent autopsy study found higher levels in the brains of Parkinson’s victims of certain PCBs found in Monsanto’s Aroclor, which was banned in 1979. The more PCBs found in the brain, the worse the brain damage. The worst three appeared to be PCBs 138, 153, and 180, all of which are significantly lower in the bodies of those eating plant-based diets (seeIndustrial Pollutants in Vegans).
So, does a vegan diet reduce the risk of Parkinson’s disease? If you watch my 3-min video Preventing Parkinson’s Disease With Diet you’ll see that every prospective study looking at dairy products and Parkinson’s disease found an increased risk associated with consumption. This may be because dairy products in the United States are contaminated with neurotoxic chemicals. Autopsy studies consistently find higher levels of pollutants in the brains of Parkinson’s disease patients, and some of these toxins are present at low levels in dairy products.
Tetrahydroisoquinoline is one such parkinsonism-related toxin found predominantly in cheese. Although the amounts of this neurotoxin—even in cheese—are not very high, the concern is that the chemical may accumulate in the brain over long periods of consumption resulting in the brain damage associated with Parkinson’s diease.
Parkinson’s Disease: Nutritional Considerations
![]()
|
Parkinson’s Disease: Nutritional ConsiderationsNutritional links to Parkinson’s disease have been identified, although the mechanisms explaining these associations are not entirely clear. Nutritional Factors in Prevention In epidemiologic studies, the following factors have been associated with reduced risk of developing Parkinson’s disease: Low–fat diets. The prevalence of Parkinson’s disease correlates with intake of animal fat,1,2 and with total and saturated fat.3 Minimizing dairy intake. The Health Professionals Follow–Up Study found a higher risk for Parkinson’s disease in men with high intakes of dairy products (roughly 3 servings per day).4 Positive associations between dairy products and Parkinson’s were found for dairy protein, dairy calcium, dairy vitamin D, and lactose, and not for other sources of these nutrients. Researchers suggest that tetrahydroisoquinolines found in dairy products may be a potential cause of this disease, due to their ability to cross the blood–brain barrier and induce degeneration of dopaminergic neurons in experimental models. The presence of dopaminergic neurotoxins, including beta–carbolines and their derivatives, pesticides, and polychlorinated biphenyls found in dairy products, may also be involved.4 Caffeinated beverages. Observational studies have found protective effects of frequent consumption of coffee or tea,5–7 although some evidence suggests that benefits are limited to men, and to women who do not use postmenopausal hormone–replacement therapy. Nutritional Factors in Treatment The most immediate nutritional concerns in Parkinson’s disease treatment include changes in the absorption rate, blood levels, and CNS uptake of L–dopa. The protein content of meals, and particularly the distribution of protein intake throughout the day, has emerged as an important consideration in the effectiveness of L–dopa for many patients.8–11 Patients with PD have a 4–fold increase in risk for weight loss of 10 lbs or more compared to age–matched controls for a variety of reasons, including dysphagia, dyskinesias, depression, and cognitive impairment; conversely, excess weight gain may occur due to an increase in sedentary behavior.12Individuals with chewing or swallowing difficulties should be referred to a speech therapist for appropriate changes in diet texture. A registered dietitian can help families plan meals that are also adequate in fluid and fiber (particularly insoluble fiber), an important concern to prevent constipation.12 Timing of protein intake The first evidence of a role for protein in modulating treatment response to L–dopa came from patient reports of deterioration of drug benefit (the ‘on/off’ phenomenon) after high–protein meals.10,11 The beneficial effects of a protein–reduced diet, or the redistribution of almost all protein to evening meals on L–dopa availability (and subsequent control of dyskinesias) have been subsequently documented in patients who experience erratic responses to levodopa therapy.8–11 In these studies, reducing protein intake to amounts as low as 10 grams/day (or 0.5g/kg body weight) resulted in an improved therapeutic response in many (though not all) individuals. Low–protein diets resulted in improvements in neurologic scoring.10 Similarly, redistributing all but 7 grams of protein intake to the evening meal resulted in improvement in the Northwest Disability and AIMS Dyskinesia Scale.9 Both low–protein diet and diets reserving protein for evening meals were associated with significant reductions in the need for L–dopa.9,10 A more recent study that both decreased protein intake to the Recommended Daily Allowance (ie, 0.8 g/kg body weight) and distributed almost all protein to the evening meal (through the use of special low–protein starches) demonstrated a similar benefit. Specifically, postprandial and total ‘off’ phases (consisting of dyskinesias and complaints of pain, parasthesias, sweating, constipation or shortness of breath) were reduced from a mean of 79 to 49 minutes, while total ‘off’ time was decreased from a mean of 271 to 164 minutes by the protein redistribution diet, reductions of 38% and 39% in ‘off’ time, respectively.8 In addition, the mid–day dosage of L–dopa was reduced in one –third patients by an average of 9%. Caution may be required because the results of protein redistribution can be so effective that an excess of L–dopa may enter the brain and trigger dyskinesia.13 A protein restriction–induced decrease in requirement for L–dopa may offer more than symptomatic benefit. It is well known that oxidative stress is central to the pathology of PD, and autoxidation of L–dopa increases oxidative stress in the substantia nigra.14 Therefore, any measures that reduce the effective dose of L–dopa may prolong the period during which patients benefit from drug therapy. In addition, high–protein meals raise blood levels of homocysteine,15 a possible risk factor for vascular disease known to be elevated in PD patients as a side–effect of L–dopa.16 Due to the risk of nutrient insufficiencies on such diets,17 multiple–vitamin–mineral supplementation has been suggested.12 Physicians interested in referring patients for a protein redistribution diet that meets both energy and micronutrient needs should contact a registered dietitian who can help patients and families to plan appropriate meals. Botanicals The seed powder of the plant Mucuna pruriens contains significant amounts of L–dopa, and has long been used in Ayurvedic (East Indian) medicine for the treatment of movement disorders.18 Although several open trials and one double blind, placebo–controlled trial demonstrated effectiveness, a report by the American Academy of Neurology concluded that there is currently insufficient evidence to support or refute the use of Mucuna pruriens.19However, considering the commercial availability of Mucuna pruriens, in addition to the growing number of East Indian immigrants to the US,20 it is not unlikely physicians may encounter patients who are using this product. Oxidative stress and Parkinson’s disease Several factors have led to the theory that oxidative stress contributes to the risk for development of Parkinson’s disease,21 possibly by causing mitochondrial decay.22 This has resulted in trials of both medications that inhibit oxidation as well as of supplements that scavenge free radicals. Vitamin E. There is good evidence that dietary vitamin E intake is inversely correlated with risk of developing Parkinson’s disease, and lower levels of vitamin E have been found in the cerebrospinal fluid of patients with the condition, when compared with patients with other neurological diseases.23However, vitamin E supplements have not been shown to be effective, either in preventing or slowing the progression of the condition.24 Coenzyme Q10. The neuroprotective effects of coenzyme Q10 (300, 600, or 100 mg/day) are under investigation for a potential role in Parkinson’s disease treatment, but statistically significant benefits have not yet been demonstrated.19 OrdersSee Basic Diet Orders chapter. A nutrition consultation would be appropriate to assist the patient in restricting protein prior to the evening hours, and restricting foods rich in vitamin B6. What to Tell the FamilyTo minimize deconditioning, patients should maintain an active lifestyle to the extent possible. Also, patients should be aware that Parkinson’s disease often causes weight loss. Family members can help reduce severe weight loss risk by providing breakfast, lunch, and between–meal snacks that are high in calories from whole grains (100% whole oats, oat bran, bulgur, barley, brown rice), fruits, 100% fruit juices, and vegetables. The family should ensure proper nutrient intake and be advised that protein deficiency is unlikely if adequate calories are consumed. Family members can improve the effectiveness of L–dopa therapy by reserving high–protein foods for evening meals. A qualified nutrition professional (eg, registered dietitian) may be helpful in accomplishing these aims.
|
Russell Henry Chittenden Tells the Truth a Century Ago
Russell Henry Chittenden Tells the Truth a Century Ago
Such narrow-minded thinking should have been stopped by 1905 when Russell Henry Chittenden, Yale University Professor of Physiological Chemistry, published his scientific findings on human protein needs in his classic book,Physiological Economy in Nutrition.2 Professor Chittenden believed Dr. Voit had cause and effect reversed: people did not become prosperous because they ate high protein diets, but rather they ate meat and other expensive high protein foods because they could afford them. One hundred years ago he wrote, “We are all creatures of habit, and our palates are pleasantly excited by the rich animal foods with their high content of proteid (protein), and we may well question whether our dietetic habits are not based more upon the dictates of our palates than upon scientific reasoning or true physiological needs.”
Professor of Physiological Chemistry, published his scientific findings on human protein needs in his classic book,Physiological Economy in Nutrition.2 Professor Chittenden believed Dr. Voit had cause and effect reversed: people did not become prosperous because they ate high protein diets, but rather they ate meat and other expensive high protein foods because they could afford them. One hundred years ago he wrote, “We are all creatures of habit, and our palates are pleasantly excited by the rich animal foods with their high content of proteid (protein), and we may well question whether our dietetic habits are not based more upon the dictates of our palates than upon scientific reasoning or true physiological needs.”
He reasoned that we should know the minimal protein requirement for the healthy man (and woman), and believed that any protein intake beyond our requirements could cause injury to our body, especially to the liver and kidneys. As he explained it, “Fats and carbohydrates when oxidized in the body are ultimately burned to simple gaseous products…easily and quickly eliminated…” “With proteid (protein) foods…when oxidized, (they) yield a row of crystalline nitrogenous products which ultimately pass out of the body through the kidneys. (These nitrogen-based protein byproducts) – frequently spoken of as toxins – float about through the body and may exercise more or less of a deleterious influence upon the system, or, being temporarily deposited, may exert some specific or local influence that calls for their speedy removal.” With these few words Professor Chittenden explained the deleterious effects of diets high in protein and meat – consequences too few practicing doctors know about today.
The First Scientific Experiments on Our Protein Needs
Professor Chittenden’s first experiment was on himself. For nine months, he recorded his own body weight, which decreased from 143 pounds (65 Kg) to 128 pounds (58 kg) on his new diet of one-third the protein that Dr. Voit recommended. Chittenden’s health remained excellent and he described his condition as being with “greater freedom from fatigue and muscular soreness than in previous years of a fuller dietary.” He had suffered from arthritis of his knee and discovered that by reducing his intake of meat his condition disappeared and his “sick headaches” and bilious attacks (abdominal pains) no longer appeared periodically as before; plus he fully maintained his mental and physical activity, with a protein intake of about 40 grams a day.
Chittenden performed valid scientific studies by collecting data on the daily dietary and urine histories of his subjects (including himself) to determine protein utilization. Because he was contradicting the known “truths” of his time, he proceeded with extreme caution with his further investigations. He organized three controlled trials with increasing demands for testing the adequacy of diets lower in protein than commonly recommended.
The first trial involved a group of five men connected with Yale University, leading active lives but not engaged in very muscular work. On a low-protein diet (62 grams daily) for 6 months, they all remained healthy and in positive nitrogen balance (more protein went into, than out of, their bodies). The second trial used 13 male volunteers from the Hospital Corps of the U.S. army. They were described as doing moderate work with one day of vigorous activity at the gymnasium. They remained in good health on 61 grams of protein daily. His final trial was with 8 Yale student athletes, some of them with exceptional records of athletic events. They ate an average of 64 grams of protein daily while maintaining their athletic endeavors, and improving their performance by a striking 35 percent. Following these studies, Chittenden in 1904 concluded that 35–50 g of protein a day was adequate for adults, and individuals could maintain their health and fitness on this amount. Studies over the past century have consistently confirmed Professor Chittenden’s findings, yet you would hardly know it with the present day popularity of high protein diets.
You have to fix the food